KNEE PAIN (a focus on anterior pain)
Anterior knee pain and dysfunction – is a common condition that affects many people. It describes pain or discomfort at the front part of the knee which is often felt under the knee cap and is associated with sounds of crepitus or clicking.
Anterior knee pain is common and presents in wide ranging populations. It is more present in females due to structural differences to males.
??CAUSES??
Possible causes of anterior knee pain include:
- patello-femoral syndrome +/- chondromalacia patella (softening or damage to the cartilage surface behind the knee cap)
- infra patella fat pad impingement and inflammation (the fat pad cushions the bottom portion of the patella/knee cap, but can be source of pain and inflammation if the knee cap continues to push into it).
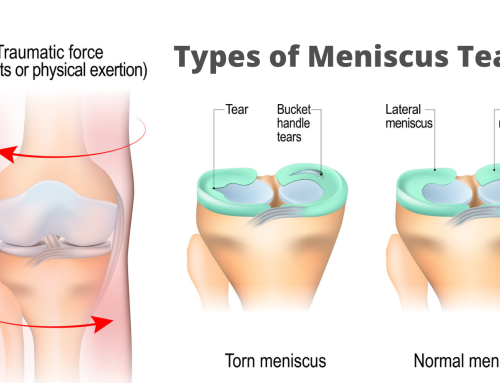
- meniscal pathology
- patella tendonopathy
- os good Schlatters (children between 13 – 18 years)
- referred from hip or back (note that slipped capital epiphysis of the hip can present as anterior knee pain)
- OCD – osteochondritis dissicens
DIAGNOSIS
As there are many possible causes to an individuals pain and dysfunction it is therefore very important to have a good differential diagnosis for accurate management. This will be performed methodically by a good therapist in their assessment to ascertain not only WHAT the cause of pain is, but also WHY you have it.
Note that the diagnosis will have a functional factor. i.e. there will normally be bias on standing knee pain, sitting (sit-stand) knee pain or functional (running, walking, stairs, etc). This will guide the focus of early rehabilitation. Rehab goals will always be guided by your assessment outcomes.
TREATMENT – treatment options will include:
- taping – it is important to “break the pain cycle” as soon as possible with anterior knee pain!! This will have an effect to decrease fear of movement, improve muscle timing and improve rehab exercise outcomes. There are multiple deloading techniques which vary slightly depending on whether fat pad or the Patella-Femoral (PF) joint is of main issue. Your therapist can teach you how to affectively self tape to find quick relief from your symptoms.
- Hip and leg strengthening – a program of strengthening exercises specific to your needs is normally required to achieve a long term outcome and change the poor mechanics which have resulted in your pain.
- Massage and soft tissue release techniques are very helpful to better align the knee
- Biomechanical re-education – a relearning of how to move is required for most people to optimise the load running through the knee. This needs to be expertly taught by an experienced therapist.
OTHER TIPS
- pillow between knees when sleeping
- shoes and footwear change – note the need for stability in feet which over pronate.
- learn how to self tape.
- avoid aggravating activities while starting rehab program
- stand in 3rd position when having to stand for long periods.
- if chronic should be reviewed every 3-6 months post successful treatment.