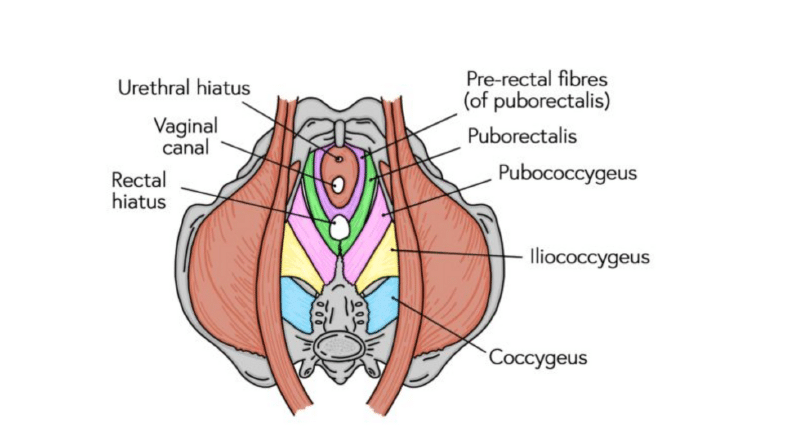
The pelvic floor is a group of muscles:
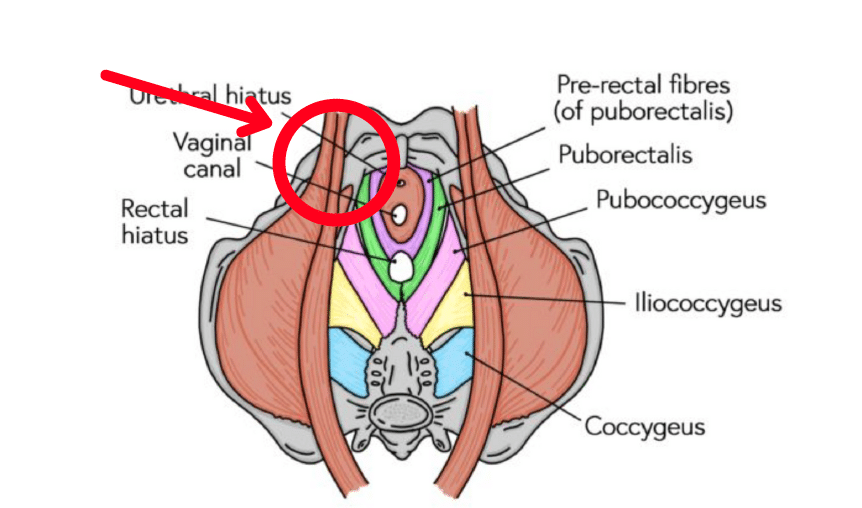
- Levator ani (made up of puborectalis, pubococcygeus and iliococcygeus)
- Coccygeus
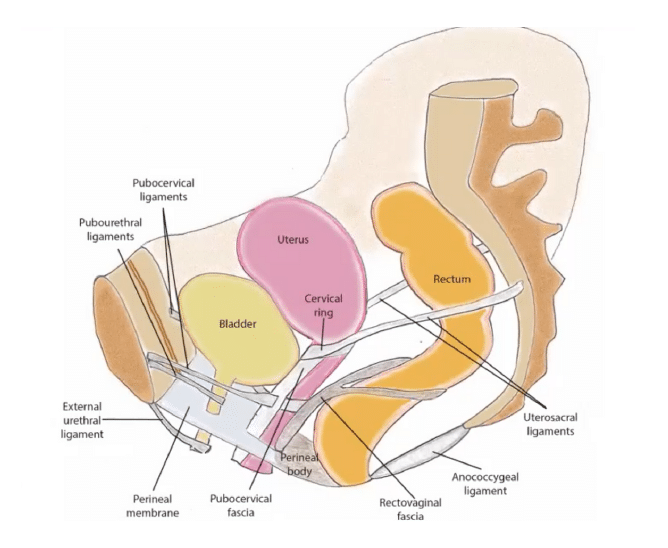
These muscles connect to the pelvic bones and spine either directly or throughconnective tissue called fascia. Together they create a bowl-like structure, forming thefloor of the pelvis. Like other areas in the body there are also ligaments providingsupport in the pelvic floor.
The pelvic floor has 2 main roles:
- Core stability, as known to be the support of the spine on the pelvis. The pelvic floorforms the base of the cylinder that makes up the deep core system.
- Support of the pelvic organs which include the bladder, rectum and uterus forwomen.
The pelvic floor contracts by
- Pulling from the back toward the pubic symphysis
- Squeezing to the middle compressing around the pelvic organs, particularly thebladder neck and rectum to aid in continence.
- Then lifting towards the head, providing a lift and support under the organs.
This functions to compress around the pelvic organs, particularly the bladder neck andrectum therefore contributing to continence.
- Dysfunctional pelvic floors can be weak, tight or both!
- Some symptoms of dysfunction can include:
- Leaking when sneezing, coughing, jumping or exercising
- Increased urgency or frequency to urinate or defecate
- Loss of continence with bladder or bowel
- Changes to sensation of the pelvic area
- Constipation for a period of time or chronic constipation
- Frequent UTI’s
- Pain with intercourse or using tampons
Dysfunction in the pelvic floor is common but is not normal. It is important tounderstand that understanding the function of the pelvic floor is the first step to treatingsymptoms and diagnosing their cause.
It is important to understand the function of a pelvic floor regardless of pregnancy. It isnever too late to assess and improve pelvic floor function when needed.
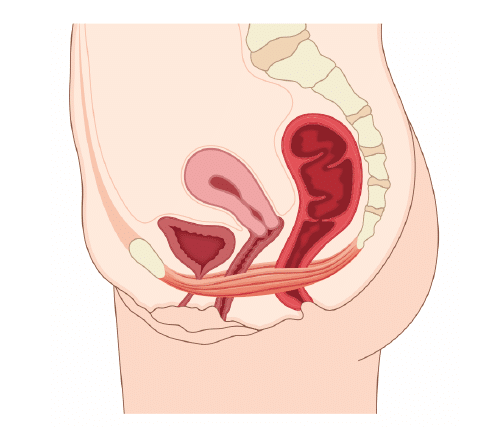
Pelvic Organ Prolapse
Prolapse means to move out of place. Prolapse of a pelvic organ is referring to thestretching or damage to the ligaments and fascia that support a pelvic organ, thereforeallowing it to move beyond its previous position.
Prolapse isn’t only caused by pregnancy. It can be linked to constant straining to pass abowel motion, increased pressures from recurrent coughs of vomiting, as well asexcessive weight.
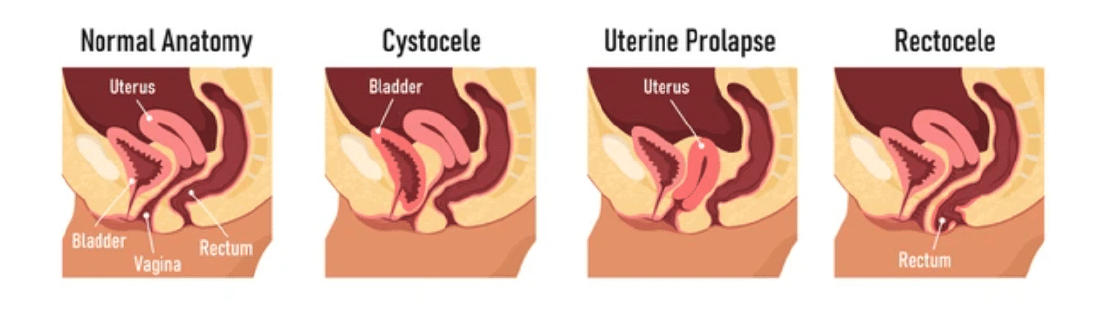
Prolapse can occur in all pelvic organs, the main types are:
- Anterior wall or cystocele, which is prolapse to the bladder
- Uterine, which is prolapse of the uterus
- Posterior wall or rectocele, which is prolapse of the rectum
There is a lot of fear associated with the word prolapse, however it is important tounderstand that it is very common, and in most cases not severe. 50% of women in fact,will experience some degree of prolapse.
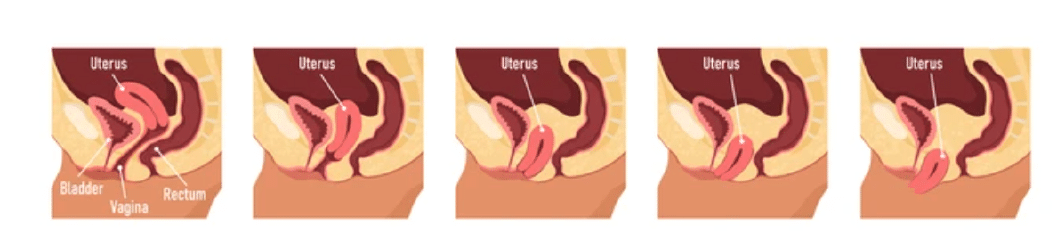
The different stages are:
- The wall/organ protrudes a small amount into the vagina, less than half of the length
- The wall/organ protrudes close to the vaginal opening or sits at the opening
- The wall/organ protrudes out of the vagina
- The wall/organ protrudes completely out of the vagina
Diagnosis of prolapse is via symptoms and an internal assessment.
Symptoms can include:
- Inability or difficulty to empty the bladder or bowel
- A slow flow or urine
- A sensation of fullness or pressure in the vagina
- A sensation of heaviness or dragging
- A bulge or swelling inside the vagina
- Bladder or bowel incontinence
Treatment can include:
- Pelvic floor strengthening
- Activity modification
- Lifestyle changes such as dietary and positions for defecation
- Pessary fitting

Only some cases will require referral for specialist assessment.
Levator Avulsion
Avulsion refers to the disconnection of the pelvic floor muscles from the pubic ramus. Inother words, the levator ani muscles can literally be pulled off the pubic symphysis boneor their attachment on the pelvic side wall. This can occur on either one or both sides.
Levator ani, particularly puborectalis and pubococcygeus, form what is known as thelevator hiatus. This is simply the sling-like support that sits under the pelvic organs. Thewider this space becomes, the less support underneath the organs and therefore theincreased risk of prolapse.
Risk factors for avulsion include:
- Advanced maternal age, first delivery
- Prolonged second stage labour (push stage)
- Major perineal tears or forceps
Treatment and management of avulsions is similar to that of prolapse and resolvesmostly around:
- Muscle training of the remaining muscle
- Pessary support
- Lifestyle modification e.g positions for defecation